
Notes from Bastia — Part 1: Where Surgical Foundations Meet Decentralized Science

Where surgical foundations meet decentralized science
Dr. Vincent Challier for SpineDAO
Introduction
My first meeting in Sainte Maxime for AO Spine basic course in 2009 put the poison of curiosity in my blood. Seeing Spine Masters on the podium confidently displaying knowledge to first year residents still resonates on me. I went to many meetings including venerable SRS, IMAST scientific societies events where well respected four minutes presentations with numbers and graphs prevail. I think these are precious because they give the most current scientific knowledge. However medium size courses are also critical, giving practical insights, a different kind of intelligence sharing system. The advent of hands-on sessions is priceless thanks to Dr. Federico Nicolosi's anatomical synthetic models that allow surgeons to practice and learn directly from the trenches with real instruments and implants.
Mille mercis to the whole NSpine team and a special thanks to my brother Dr. Joseph Cristini and his gang of marvelous humans who made this possible under the sky of heavenly Corsica.
This series will deal with the impressions, the notes that I gathered during this wonderful journey. I was not able to attend to all sessions, apologies, but I wanted to share my feelings of simple human in front of cutting edge technology, innovations and most important: Humanity.
The View from Corsica
There is something quietly fitting about staging a meeting on the future of spine surgery in Bastia. Corsica is a Mediterranean crossroads — French in administration, Italian in temperament, geographically nearer to Tuscany than to Marseille — and the Southern European Spine Summit held there from May 14th to 16th, 2026, was itself a crossroads of another kind. Three days, three thematic arcs, and a faculty that read like an atlas: France, Italy, Spain, Portugal, Greece, Germany, Monaco, the Netherlands, Switzerland, the UK, Turkey, Ukraine — and from further afield, the United States, Brazil, Argentina, Mexico, Japan, India, Indonesia, Vietnam, and South Africa.
The venue itself — the Institut Régional d'Administration de Bastia, a serious-looking civic building above the port — was a deliberate choice. NSpine has never gone in for the conference-resort aesthetic. The room was a working amphitheatre, the chairs were filled, and from the first session the tone was set: this would be a meeting about substance, not stagecraft.

Day 1 — Plenary: Degenerative
The first day opened with the bread-and-butter of spine practice: lumbar approaches for degenerative disease. The moderators — Samir Smajic, Bronek Boszczyk, and Guillaume Lonjon — set up a session that moved methodically through the central tensions of the modern lumbar OR: direct versus indirect decompression, anterior versus posterior, fusion versus motion preservation, MIS versus endoscopic.
Bronek Boszczyk — Multilevel ALIF for complex deformity reconstruction
It was fitting that Bronek Boszczyk, NSpine's founder and Head of Paediatric Spine Surgery at Aschau Orthopaedic Hospital, took one of the first slots of the conference. His subject — multilevel anterior lumbar interbody fusion for complex deformity reconstruction — is a topic that, in lesser hands, can become a parade of personal techniques. Boszczyk did the opposite.
His slide showed two things side by side: an axial anatomical cross-section of the lumbar region, with the great vessels, the bowel and the surrounding fascial planes mapped out in colour; and the standing biplanar radiographs of a patient with a significant sagittal and coronal deformity. The caption read simply: "Necessity for range of access techniques."
The argument behind that slide is one that doesn't get said often enough at podium level. At every lumbar level, the vascular and visceral relationships shift. The bifurcation of the great vessels sits where it sits. The peritoneum reflects where it reflects. A surgeon who has one approach in their hands is, by definition, the wrong surgeon for the multilevel reconstruction — because a single approach cannot honour the anatomy of every level on the same patient. ALIF at L5–S1 is not ALIF at L4–L5, and neither is ALIF at L3–L4. Each level is its own surgical decision.

The second slide drove the point home with a quiet act of credit. Boszczyk paid tribute to Dr. Sal Brau of Los Angeles — a vascular access surgeon with more than 3,000 anterior approach procedures to his name, capable of completing single-level access in under ten minutes and double-level in under twenty. The implicit message, delivered without theatre, was about humility and team composition. For the most complex multilevel reconstructions, the modern answer is not "I do it all myself." It is "I work with someone better than me at access."

This is the kind of opening tone that distinguishes NSpine from more vendor-driven meetings. The first technical talk of the conference wasn't a product showcase. It was a senior surgeon telling a room full of peers that mastery, at a certain point, looks like collaboration.
Patrick Tropiano — Strategy for lumbar total disc replacement revision and salvage
The 9:20 slot belonged to Patrick Tropiano, the Marseille spine veteran whose decision algorithm filled the screen behind him. "Indications for Anterior Revision" the slide read — followed by a decision tree that any spine surgeon will recognise as one of the genuinely difficult problems of the field. When a lumbar total disc replacement fails, what next?
Tropiano's algorithm begins with the patient. High-risk patients — defined here not by comorbidity but by the nature of the failure — are routed to anterior revision, the more demanding path. The logic is counter-intuitive at first glance, until you remember that the prosthesis itself sits anteriorly: if the failure is at the implant, the revision must reach the implant. From the anterior branch, the algorithm forks again. If exposition is possible without vascular complication and anchorage quality is preserved, the surgeon proceeds. If exposition is incomplete or anchorage difficult — the polite phrase for "the previous approach has welded the retroperitoneum together" — the strategy pivots to interbody fusion, with sub-decisions about polyethylene migration, miscentering, plate displacement, and complete revision.
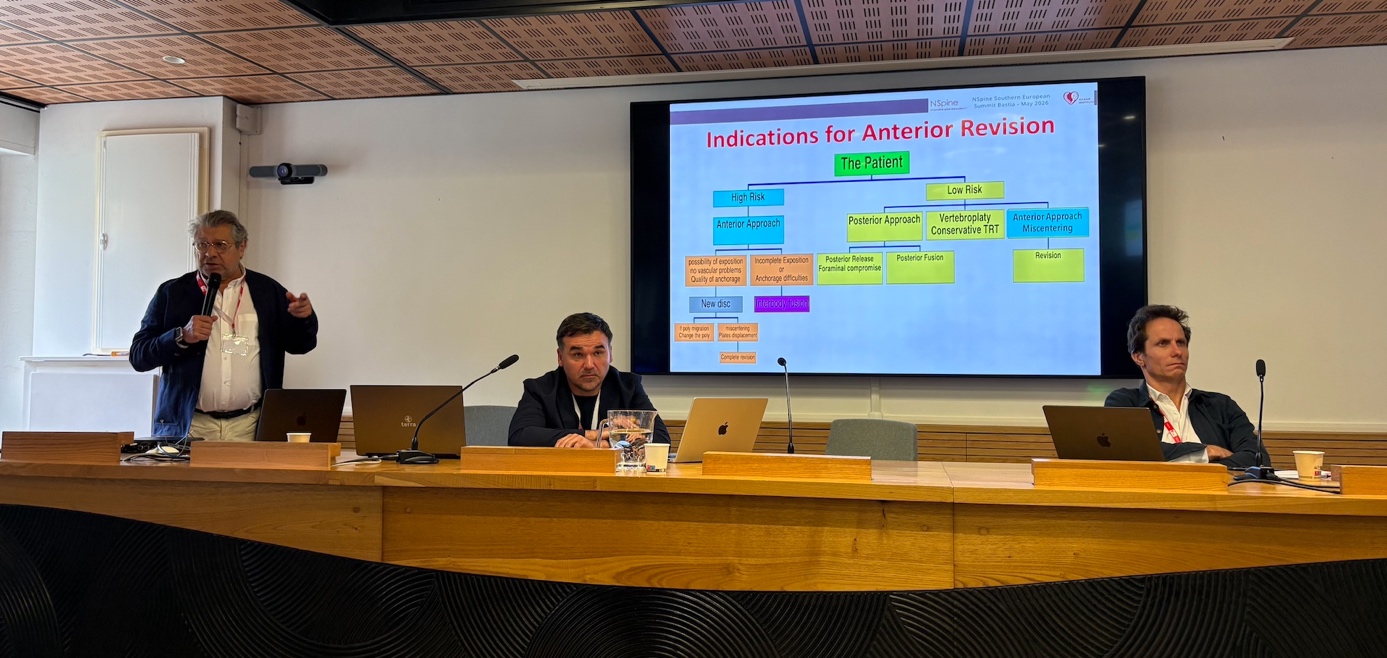
Low-risk patients take the more conservative routes: posterior release for foraminal compromise, vertebroplasty or conservative management where appropriate, and anterior revision only where miscentering of the prosthesis itself demands it.
It is the kind of slide that does not survive being read once. But the point, beyond the specifics, was this: TDR revision is the surgical problem that everyone secretly wants someone else to handle, because the prior anterior approach has already cashed in the easy access window. Tropiano's framework — and the calm with which he presented it — was a reminder that in revision work, having a process matters more than having a preference. It also reinforced Boszczyk's argument from ten minutes earlier: the moment you are revising a previous anterior surgery, the access-surgeon question is no longer optional.
The Room
A glance over the lectern, somewhere between Tropiano and Khalifé, gave the meeting's social geography away. The amphitheatre was full. Red lanyards across every chest. Laptops open on knees — some taking notes, some quietly running their own image analysis on a case they had been turning over for the past hour. The faces were Mediterranean, Northern European, South Asian, East Asian, Latin American. It was a working room in the genuine sense of the phrase, the kind of audience where the questions afterwards are usually better than the talks.

Marc Khalifé — Decision making in direct vs. indirect decompression in fusions
If Tropiano represented the senior Marseille generation, Marc Khalifé represented the next wave: Paris-based at Hôpital Européen Georges Pompidou and Hôpital Necker, affiliated with Université Paris Cité, and squarely focused on one of the most contested decision points in contemporary lumbar surgery.
Direct versus indirect decompression in fusions is the lumbar question of the past decade. The classic teaching is straightforward: if a nerve is compressed, the surgeon decompresses it directly. Open the canal, remove the bone or ligament that is pinching the root, see it move, close the patient. But the rise of minimally invasive and lateral approaches has opened a second route. With ALIF, LLIF, OLIF and their cousins, restoring disc height with a tall enough interbody cage pulls the ligamentum flavum taut, re-tensions the annulus, distracts the foramen and, in many cases, decompresses the nerve indirectly — without ever touching the posterior elements.

The appeal is obvious. No muscle stripping. No facet violation. Less blood. Faster recovery. But indirect decompression is not an article of faith; it is a technique that works in some patients and fails in others, and Khalifé's talk was about predicting which patient is which. Severe central stenosis with calcified disc material, symptomatic facet hypertrophy, far-lateral disc herniations, severe foraminal narrowing where the bony architecture itself is the obstacle — these are the cases where height restoration alone will not deliver, and where a hybrid approach (lateral interbody combined with limited posterior decompression) often outperforms either pure strategy.
Khalifé's framing was deliberately practical: imaging predictors, symptom patterns, patient-by-patient reasoning rather than philosophy-of-surgery declarations. It is the kind of talk that, ten years ago, would have been impossible to give because the data did not yet exist. Now it exists, and it is changing how spine surgeons think.
Taken together, the three opening talks — Boszczyk on access for primary multilevel work, Tropiano on access when something has already gone wrong, Khalifé on whether to decompress at all — formed a tight conceptual triplet. Three different surgeons, three different countries, three different career stages, all circling the same underlying question: in a field where every approach has its evangelists, how do you make the decision in front of you, for the patient in front of you, without falling in love with your own technique?
The slot pointed toward an answer, and toward a thread that would run through the rest of the conference.
Anton Denisov — ALIF as an alternative to posterior surgery in patients with moderate sagittal imbalance
The title slide alone was worth pausing on. Three logos sat across the top: NSpine, SpineDAO, and Causse Clinic. The speaker line read, in four parts: Anton Denisov, MD, MBiostat. Spinal Surgeon at Causse Clinic (Girona, Spain). Senior Biostatistician at The Taylor Collaboration (USA). Clinical Investigator at SpineDAO. It was the first time at the meeting that the SpineDAO acronym had appeared on a podium slide — and it appeared not at a DeSci showcase, but in the middle of a clinical talk on sagittal balance correction, given by a surgeon who is also a biostatistician. The signal was easy to miss and impossible to overstate.

The talkitself was a clinical argument with citations, and a refreshingly honest one.Denisov anchored it in four references that together form the backbone ofmodern sagittal-balance evidence:
- Pellisé et al., Eur Spine J 2015 — sagittal imbalance is a major driver of disability and HRQOL loss, often exceeding many other chronic diseases.
- Spanomitis et al., Eur Spine J 2017 — once the spine is fused, postoperative alignment matters more for HRQOL than preoperative alignment.
- Schwab et al., Spine 2018 — under-correction, particularly of SVA and PI–LL mismatch, drives worse outcomes; over-correction offers no HRQOL gain and may add complications.
- Formica et al., Eur Spine J 2021 — ALIF supports near-physiological sagittal alignment through distal lordosis restoration.
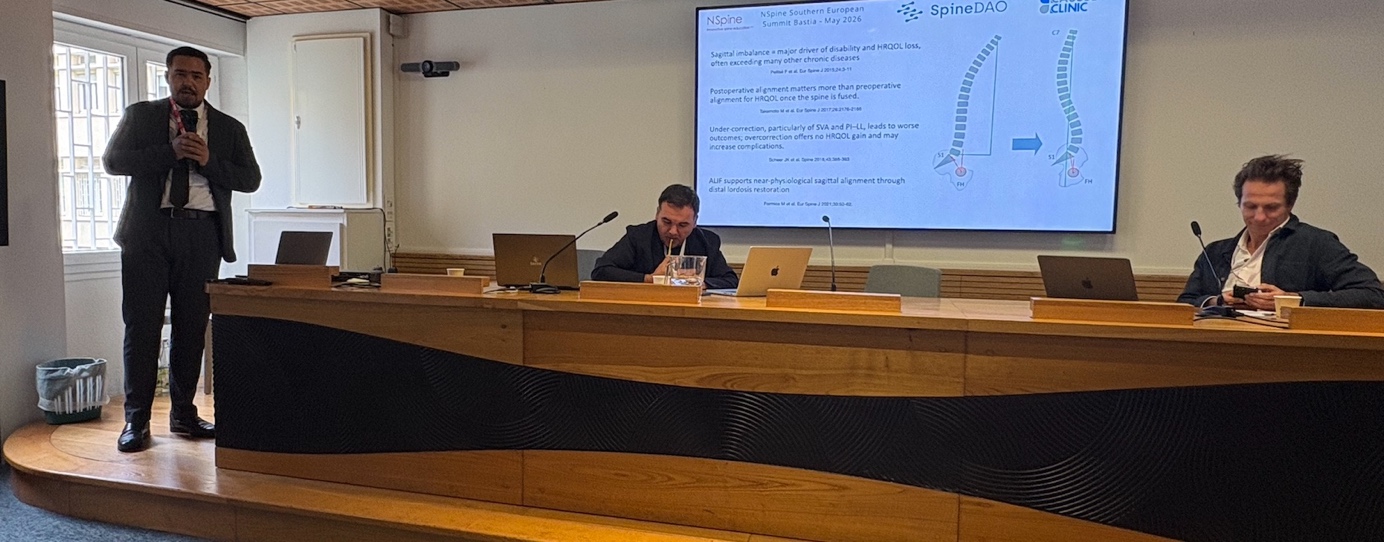
The clinical argument followed cleanly. For patients with moderate — not severe — sagittal imbalance, the field has historically reached for posterior corrective work: three-column osteotomies, multilevel posterior column releases, long fusions. These are powerful but morbid procedures. ALIF offers a different lever. The majority of physiological lumbar lordosis lives in the two distal segments, L4–L5 and L5–S1, and ALIF restores that distal lordosis directly through disc-height restoration with a hyperlordotic cage.
The window of acceptable correction is narrow — Schwab's data make that explicit — and the under-/over-correction asymmetry argues for precision, not for maximum manoeuvre. ALIF, used judiciously, can deliver that precision in the moderate-imbalance patient while avoiding the morbidity of the larger posterior operation.
Denisov's Key messages slide reduced the position to four lines:
The last line is the one to take home — and it is also, not coincidentally, the line that explains why this surgeon, working at the intersection of clinical practice and biostatistics, has thrown his lot in with SpineDAO. Individualised strategy depends on data. Not the polished, finished-paper, tip-of-the-iceberg data that appears in journals after a two-year peer-review delay, but the granular per-case data that lives on hard drives in clinics across the world.

The SpineDAO badge on Denisov's title slide was, in retrospect, a quiet announcement. The DeSci conversation had begun, and it had begun inside a sagittal-balance talk on Day 1. By the time the same speaker would return to the podium on Day 3, presenting the methodology and preliminary results of the SpineBase TLIF-BAYES ongoing research campaign.
Samir Smajic — Prone vs. lateral decubitus single-position LLIF and posterior
The 9:50 slot brought a different rhythm. Samir Smajic, a German spine surgeon presenting cases watermarked St. Josef-Krankenhaus, came to the lectern with one of the busier questions in contemporary MIS practice: single-position surgery, and specifically the choice between prone and lateral decubitus as the starting position when the plan includes both lateral interbody work and posterior fixation in a single anaesthetic.
Single-position surgery is, on its surface, a logistical problem. The classical sequence — lateral lumbar interbody fusion in lateral decubitus, then flip the patient to prone for posterior fixation — adds time, adds the risk of repositioning errors, and accumulates the small complications of double-positioning. The single-position alternatives compress this into one set-up: either prone LLIF (the lateral interbody work performed with the patient kept prone, then the same prone position serves for the screws), or lateral decubitus throughout (LLIF first, then percutaneous posterior fixation from the same side, which is technically harder and unforgiving in the obese patient).
Smajic's central slide — a decision tree titled "Decision Tree Based Primarily on (Patho)Anatomical Considerations" — had green nodes for clinical inputs (L2–4 only, L4/5 included, L5/S1 included, corridor vessel-psoas/plexus, high iliac crest, Mickey Mouse configuration, obesity, "ALIF reasonable?"), blue nodes for resulting procedures, and a branching logic that ended in real-world combinations: prone LLIF, OLIF, OLIF L(2)4/5 plus lateral ALIF L5/S1, TLIF L(2)4–S1, and various salvage and hybrid paths.
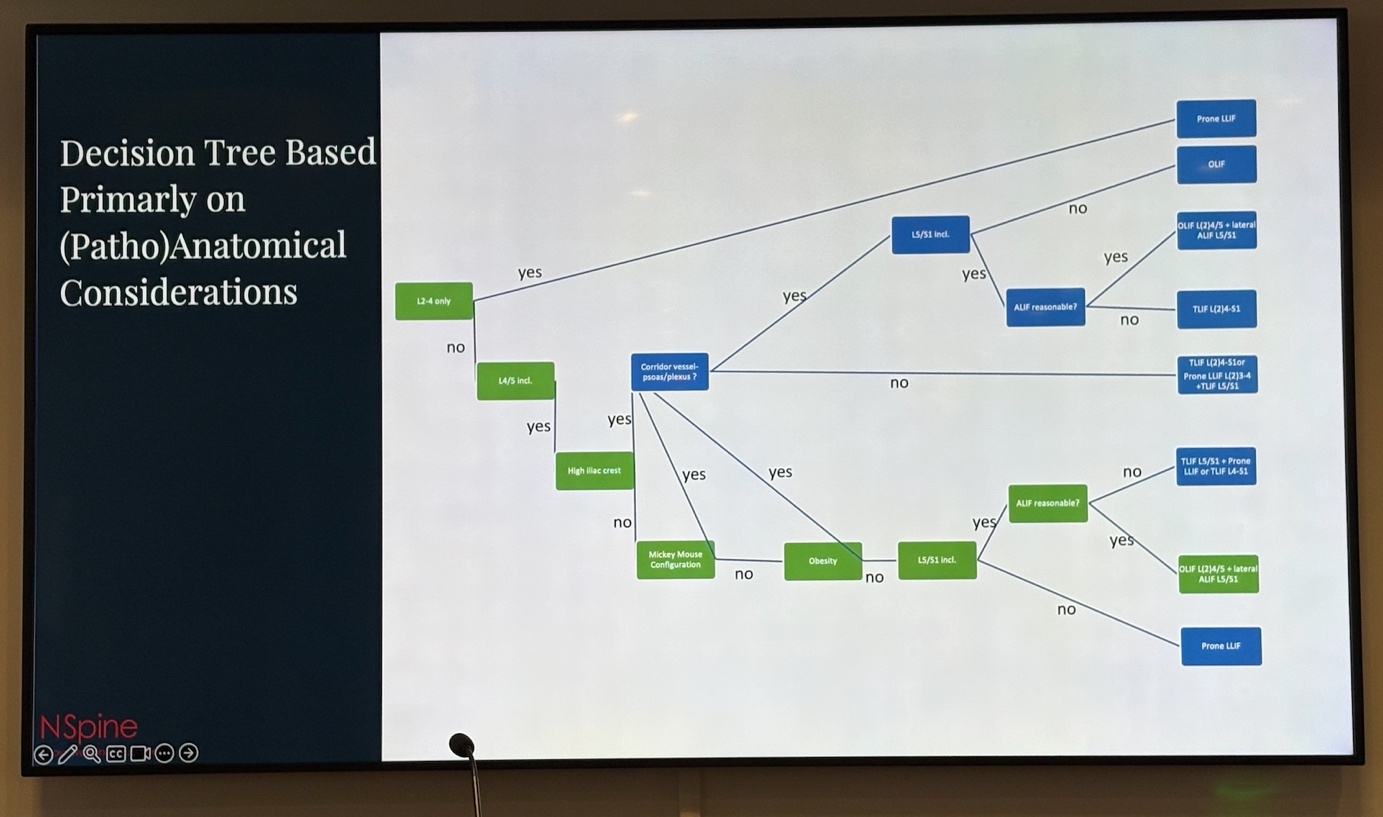

This was a different kind of decision-making than the binary debates of the earlier triplet. Boszczyk, Tropiano and Khalifé had each presented a question and developed it; Smajic was presenting the plumbing — the actual operational logic a surgeon walks through to translate a complex case into an executable plan. The slide was less a teaching tool than an artefact of clinical practice. One could imagine it taped to the back of an OR door.
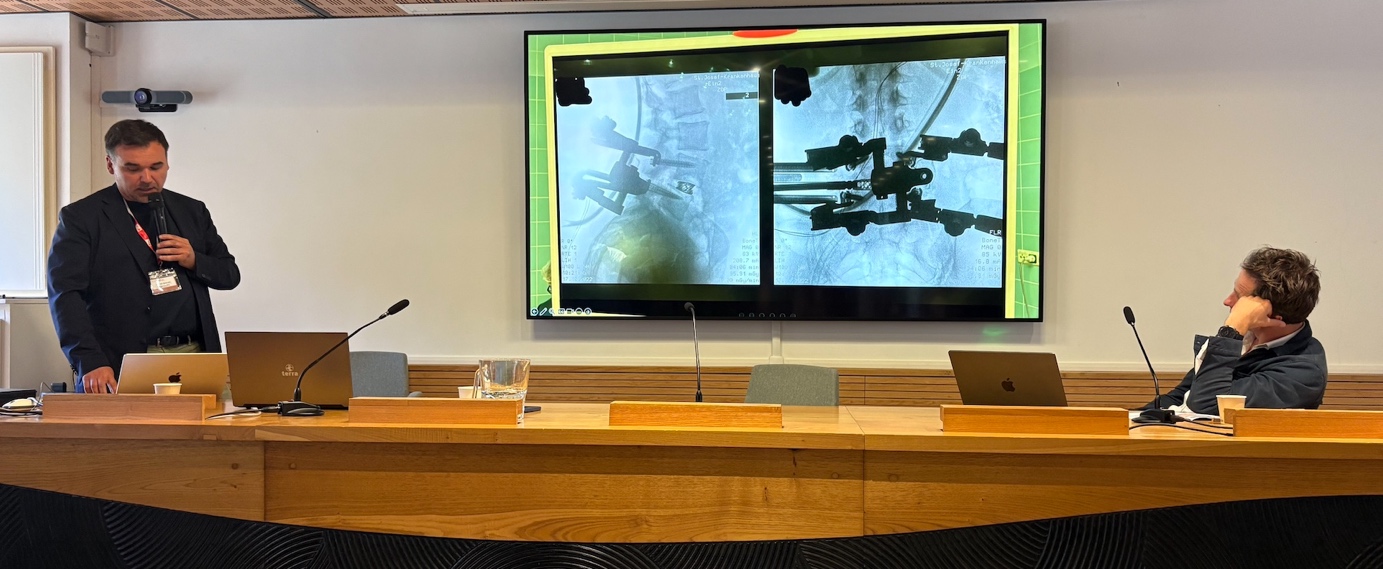
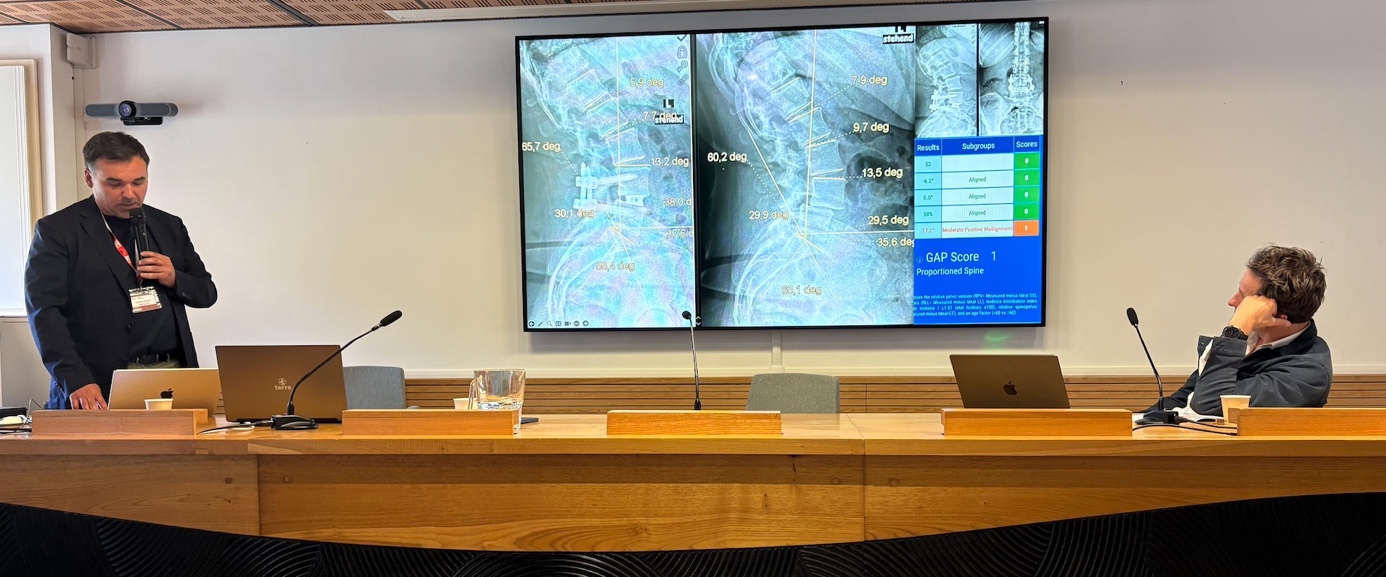
The supporting case material did the work it had to do. Intraoperative fluoroscopy from his unit showed pedicle screw placement during prone LLIF — screws going in from above while the lateral interbody corridor remained accessible at the side. Postoperative imaging walked through measured outcomes against the GAP score (Yilgor and colleagues' Global Alignment and Proportion scale, the now-standard mechanical-complication predictor in deformity work). A worked example landed at GAP 1 — proportioned spine — with four of five subgroup measures aligned and one sitting at moderate positive malalignment. Not perfection; rather, the language modern deformity science uses for good enough on the metrics that predict mechanical durability.
And then, at the very end of the deck, came the slide nobody in the room was expecting. The takeaways slide, instead of a bullet list, displayed a sleekly Photoshopped tribal arrangement of shirtless, tattooed MMA fighters under stage lighting. The text behind the figures was partially obscured but the framing was unmistakable: in this modern era… trained fighter… patient need. The room responded the way a room of senior surgeons usually responds to that kind of move — with the small, knowing laugh that says yes, we get it. The point, beneath the swagger, was serious. Single-position surgery is not the operation for an occasional lateral surgeon.

Ignacio Moya — Motion preservation in 2026
If the nine o'clock hour had been about how to fuse better, the 10:00 slot pulled in the other direction. Ignacio Moya, from Spain, used his ten minutes to make the case for not fusing at all — when the indication permits — and devoted much of the talk to the Intra Spine device from Cousin Spine, a dynamic interspinous stabilisation implant designed to preserve segmental motion rather than abolish it.
Motion preservation has had a difficult fifteen years in the lumbar spine. The early interspinous devices — X-Stop most famously — over-promised, under-delivered, and in several cases ended up withdrawn from the market. The reaction was nearly a decade of broad skepticism about the entire category. Moya's argument, framed against that history, was that the category had not failed because the idea was wrong; it had failed because the implants had been wrong. The Intra Spine, with its silicone wing geometry seated in the interspinous space, is designed around a more biomechanically faithful conception of what the motion segment is actually doing — distracting the posterior elements, unloading the facets, and maintaining a controlled range of segmental movement rather than locking the segment in extension.
In carefully selected patients — moderate central or foraminal stenosis with preserved disc height, no overt instability, neurogenic claudication rather than frank radiculopathy — the indication, in Moya's account, is once again defensible. The talk was a reminder that motion preservation is not an ideology. It is a set of indications that the field is slowly relearning how to honour, and that — given the morning's earlier emphasis on individualised strategy — sits naturally inside the same intellectual frame as Denisov's biostatistical pragmatism and Khalifé's data-driven decompression decision tree. Fuse the patient who needs to be fused. Don't fuse the patient who doesn't.
Hao-Hua Wu — Sagittal balance restoration: when is fusion not enough?
The 10:10 slot belonged to Hao-Hua Wu, one of the more prolific US voices in contemporary adult spinal deformity. The title — Sagittal balance restoration: when is fusion not enough? — pointed at the question every revision surgeon eventually confronts, and that sits at the other end of the lever from Moya's motion-preservation pitch.
The Schwab data Denisov had cited an hour earlier — that under-correction of SVA and PI–LL mismatch is the primary mechanical predictor of bad outcomes in ASD — is the same evidence base that, on the operating side of the equation, drives the decision to add an osteotomy, extend a construct, or revise a previously fused segment that has aged badly. The session sat in productive tension with the morning's broader motion-preservation and MIS arguments. The same field that is learning to fuse less, in the right patient, is also learning to correct more decisively when fusion is the right answer. Both lessons emerge from the same source: better data, better stratification, and better honesty about which patients are actually being helped by which operation.
Shawn Venter — From MIS to endoscopic fusion surgery
Shawn Venter, the South African contribution to a Mediterranean meeting, took the 10:20 slot to walk through the steepest part of the modern MIS curve: the transition from minimally invasive fusion to endoscopic fusion, and specifically the rise of UBE TLIF — unilateral biportal endoscopic transforaminal interbody fusion.
UBE is the procedure that has spent the past five years climbing the diffusion-of-innovations curve faster than any other technique in the lumbar arsenal. Two small portals — one for the endoscope, one for instruments — with continuous saline irrigation maintaining the working cavity; direct endoscopic visualisation of the dura, the traversing root, the disc; and a learning curve that is, by general consensus, vertical. Venter, working out of the Spine Centre, is one of the surgeons who has been on the steep end of that curve, and his deck reflected the perspective of someone who had already done the work.

The talk displayed an incredible and inspiring intraoperative video — UBE TLIF in progress, two instruments converging on the operative cavity through a couple of centimeter-scale skin incisions, the interbody cages waiting just outside the field. The visual argument was the one no slide can really make in words: this is what the back of the patient looks like at the end of a fusion that, a decade ago, would have left a much larger scar.
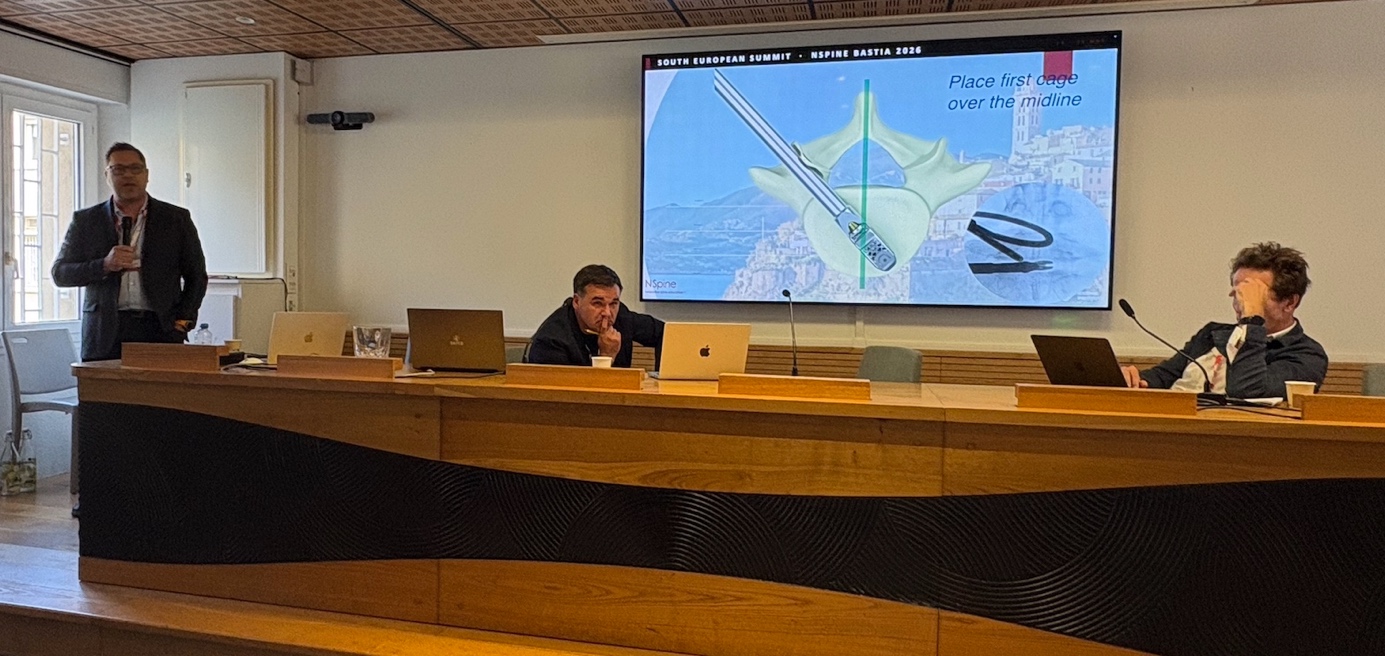
Venter exhibited a technical note that the cage-placement subspecialists in the room would have appreciated: place first cage over the midline. The technique illustration — a 3D vertebral schematic with cage trajectory overlaid on the Bastia skyline — was followed by a fluoroscopic still showing a centred, well-positioned interbody construct under live imaging.

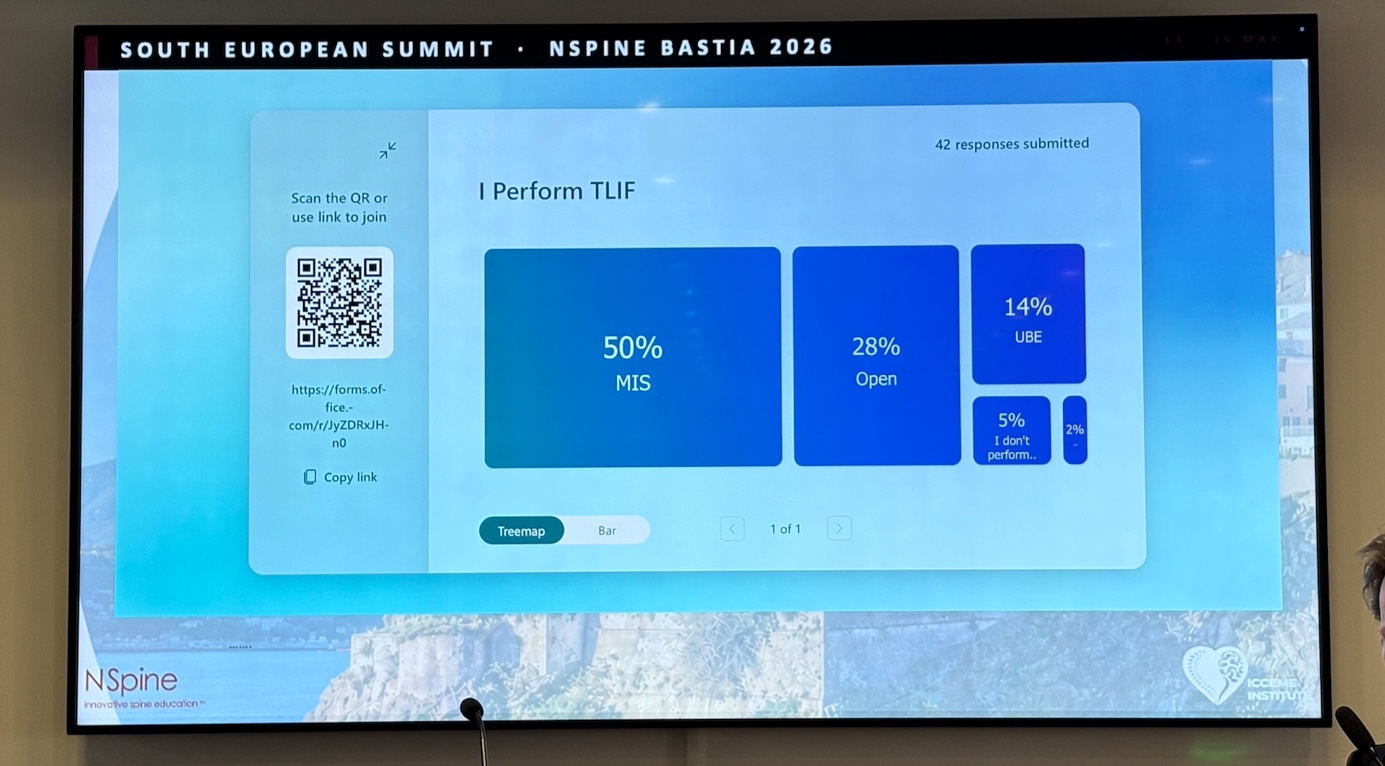
But the most interesting moments of the talk were the live polls. The first asked the audience: I perform TLIF…
The room, sampled at forty-two respondents, broke down as: 50% MIS, 28% Open, 14% UBE, 5% don't perform, 2% other. Read that distribution carefully. Half the surgeons in the room had moved to a minimally invasive TLIF as their default. More than one in seven had moved further still, to UBE. The traditional open TLIF, while still substantial, was no longer the majority view.
The second poll asked the inverse: I DO NOT perform UBE TLIF because:
The dominant answer, by a wide margin, was 51% equipment and theatre setup. The other reasons trailed at much smaller magnitudes: 12% radiation and imaging workflow, 12% patient selection limitations, 12% dural tear management, and — one has to admire the honesty — 9% I'm too old :)
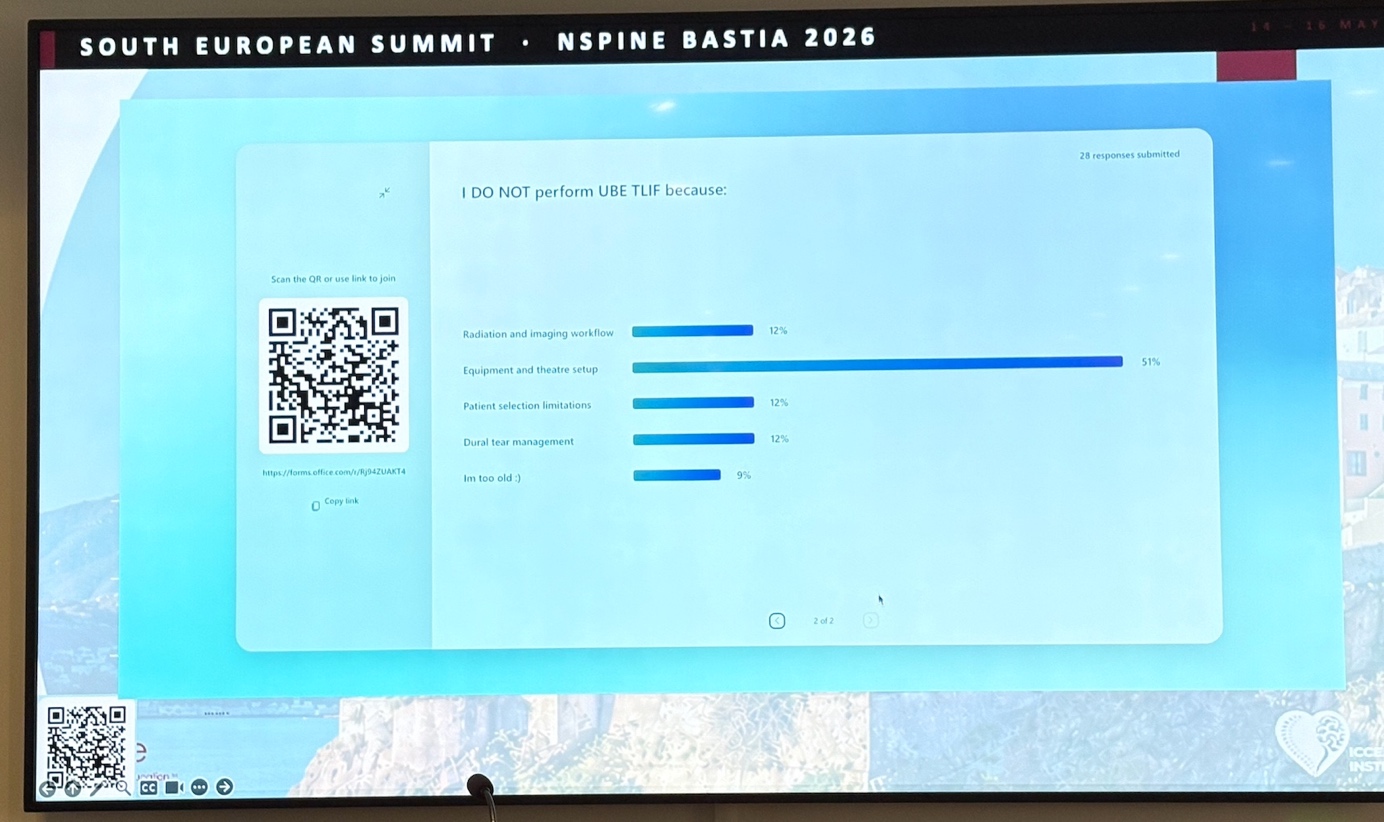
This is the kind of finding that does not appear in any randomised controlled trial, and that any registry would struggle to capture. The barrier to UBE adoption is not patient outcomes, not surgeon skill, not evidence. It is the operating theatre itself: the irrigation pumps, the endoscopic stack, the C-arm workflow, the OR nurses trained in fluid management. It is, in a word, infrastructure. And infrastructure is the kind of problem that responds well to collective, federated effort.
Guillaume Lonjon — Controversy debate: MIS fusion vs endoscopic decompression alone
The 10:30 slot, the closing item of the morning's plenary, was a debate slot. The title — MIS fusion vs endoscopic decompression alone — was the kind of formal controversy item that NSpine occasionally programs to keep the audience honest, and the surgeon defending the decompression alone side was Guillaume Lonjon, a Montpellier-based orthopaedic spine surgeon.
Lonjon opened with a slide titled, with disarming directness, Who I am. Specialty: endoscopic surgeon. Date of first UBE case: April 2022. UBE exclusif — exclusively endoscopic practice — since January 2023. Personal series: more than six hundred UBE cases, plus forty uniportal. Maximum step achieved on the published UBE procedural-difficulty classification (Correa Valencia, 2022): step 7 — the most advanced rung, covering cervical over-the-top approaches and thoracic calcified herniations. And, at the institutional level, more than seventeen hundred UBE cases in the center, with UBE accounting for 75% of the surgical mix.

The payoff came on the conclusion slide, and the answer was less polemical than the debate format would have led one to expect. Lonjon's position, in the case of spondylolisthesis, was that decompression, stabilisation, and fusion are complementary — not antagonistic — and that the choice between them can be reduced to a three-criterion score:
Criteria2 points1 point0 pointsAge<6060–75>75Instability—yesnoOsteoporosis—noyes
Treatment by score: 3–4 points → TLIF (fuse) | 1–2 points → dynamic stabilisation | 0 points → decompression alone
That is, the young, unstable, non-osteoporotic patient gets fused. The old, stable, osteoporotic patient gets decompressed and sent home the same week. The middle is bridged by dynamic stabilisation. The framework is a model of practical clinical reasoning, and it deliberately disarms the binary framing of the debate. Decompression alone is not an alternative philosophy to fusion. It is a different treatment, for a different patient.

This was the second time in the same morning that a surgeon had closed a talk with a scoring tool rather than a slogan. Smajic had done it with his anatomy-driven decision tree; Lonjon did it now with this clinical score. The two artefacts differ in domain but rhyme in spirit. In a meeting that would, over the coming two days, increasingly explore the role of data and federated infrastructure in spine practice, the through-line of the morning was already visible by 10:30: we score, we stratify, we individualise, we record.
It was as good a hand-off as the Innovation & Robotic block at 11:00 could have asked for — and a quiet preview of the analytic posture that would dominate the rest of the conference.
To be continued…
Stay tuned for Part 2: Innovation, Robotics, and SpineDAO's formal entry onto the podium.















%20Medium.png)


.png)